Aceruloplasminemia is a NBIA disorder that is characterized by iron accumulation in both the brain and visceral (internal) organs.
SYMPTOMS
Symptoms of aceruloplasminemia are typically found in individuals ranging from age 25 to older than age 60.
Common symptoms include:
Retinal degeneration (deterioration of the retina in the back of the eye)
Diabetes
- Causes individuals to have high blood sugar
- Can result in symptoms such as frequent urination, increased thirst and increased hunger
- Caused by iron accumulation and damage in the pancreas, where insulin is made
Ataxia (uncoordinated, jerky movement of the muscles)
- Gait ataxia (jerky, unsteady walking)
- Limb ataxia (jerky, unsteady movement)
- Dysarthria
- Difficulty using or controlling the muscles of the mouth, tongue, larynx or vocal cords which are used to make speech
- This can make a person’s speech difficult to understand in several different ways, including stuttering, slurring, or soft or raspy speech
- Can result in reduced vision
- Sometimes called “dancing eyes”
Involuntary movement
- Face and neck dystonia (involuntarily muscle contraction and spasms)
- Blepharospasm (sustained, forced, involuntary closing of the eyelids)
- Grimacing
- Chorea (brief, irregular muscle movements that occur involuntarily and cannot be controlled by the person experiencing them)
Parkinsonism (symptoms similar to Parkinson’s disease)
- Tremors (shaking)
- Hypokinesia (decreased muscle movement)
- Rigidity (stiffness)
- Akinesia (cannot initiate muscle movement―cannot get started)
Cognitive (mental) decline
- Generally seen in individuals older than age 50
- Can lead to dementia
Anemia
- A decrease in the number of red blood cells or a decrease in the quantity of hemoglobin in the blood
- Individuals may show anemia before a diagnosis of diabetes or neurologic problems is made
Psychiatric problems
- Depression
CAUSE/GENETICS
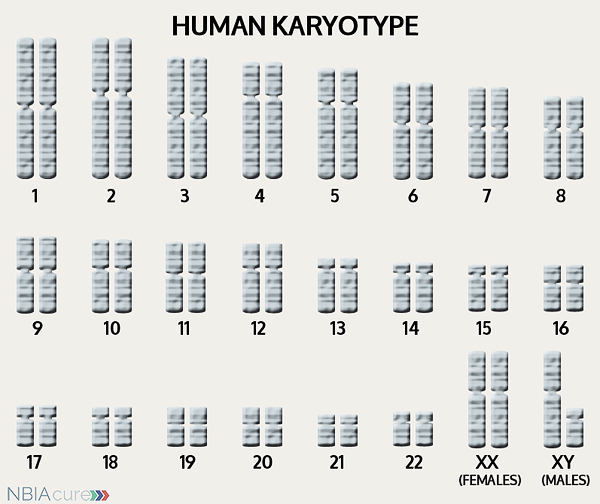 The human body is made up of millions of cells. Inside every cell there is a structure called DNA, which is like an instruction book. DNA contains detailed steps about how all the parts of the body are put together and how they work. However, DNA contains too much information to fit into a single “book,” so it is packaged into multiple volumes called chromosomes. Humans typically have 46 total chromosomes that are organized in 23 pairs. There are two copies of each chromosome because we receive one set of 23 chromosomes from our biological mother and the other set of 23 from our biological father. Chromosomes 1-22 are called autosomes and the last pair is called the sex chromosomes because they determine a person’s gender. Females have two X chromosomes and males have one X and one Y.
The human body is made up of millions of cells. Inside every cell there is a structure called DNA, which is like an instruction book. DNA contains detailed steps about how all the parts of the body are put together and how they work. However, DNA contains too much information to fit into a single “book,” so it is packaged into multiple volumes called chromosomes. Humans typically have 46 total chromosomes that are organized in 23 pairs. There are two copies of each chromosome because we receive one set of 23 chromosomes from our biological mother and the other set of 23 from our biological father. Chromosomes 1-22 are called autosomes and the last pair is called the sex chromosomes because they determine a person’s gender. Females have two X chromosomes and males have one X and one Y.
If DNA is the body’s instruction book and it is stored in multiple volumes (called chromosomes), then genes would be the individual chapters of those books. Genes are small pieces of DNA that regulate certain parts or functions of the body. Sometimes multiple genes (or chapters) are needed to control one function. Other times, just one gene (or chapter) can influence multiple functions. Since there are two copies of each chromosome, there are also two copies of each gene. In some gene pairs, both copies need to be expressed (or turned on) in order for them to do their job correctly. For other genes pairs, only one copy needs to be expressed.
When a single cell in the human body divides and replicates, its DNA is also replicated. This replication process is usually very accurate but sometimes the body can make a mistake and create a “typo” (or mutation). Just like a typo in a book, a mutation in the DNA can be unnoticeable, harmless, or serious. A mutation with serious consequences can result in a part of the body not developing correctly or a particular function not working properly.
In the case of NBIA disorders, changes in certain genes cause a person to develop their particular type of NBIA. Changes in these NBIA genes lead to the groups of symptoms we observe, although we do not yet understand how the changed genes cause many of these findings. CP is the only gene known to cause aceruloplasminemia. CP’s main job is to tell the body’s cells how to make a protein called ceruloplasmin, which carries copper in the blood and plays a role in iron metabolism (breakdown).
As mentioned earlier, humans have a total of 23 pairs of chromosomes. Half of these chromosomes are passed down (or inherited) from the biological mother and half from the biological father. The way in which a gene change is passed down from parents to child varies from gene to gene. The CP gene that is altered in those with aceruloplasminemia is inherited in an autosomal recessive manner.
“Autosomal” refers to the fact that the CP gene is located on chromosome 3, which is one of the autosomes (chromosome pairs 1-22). Since the sex chromosomes are not involved, males and females are equally likely to inherit a gene change located in the autosomes. “Recessive” refers to the fact that a gene change must be present in both copies of the CP gene for a person to have aceruloplasminemia. If an individual has only one CP gene change, then they are called a “carrier” for . Carriers do not have health problems related to the gene change and often do not know they carry a recessive gene change. However, if two carriers have a child together, then there is a 25% chance that they will both pass on their recessive CP gene changes and have a child with .
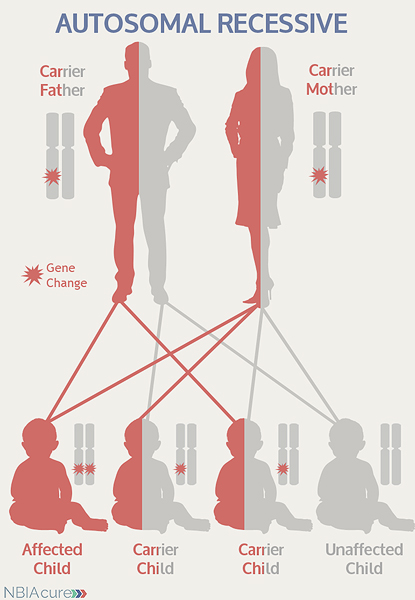 As seen in the image to the left, in a pregnancy between two aceruloplasminemia carriers:
As seen in the image to the left, in a pregnancy between two aceruloplasminemia carriers:
- There is a 25% chance of the child having aceruloplasminemia
- There is a 50% chance that the child will be a carrier like his/her parents
- There is a 25% chance that the child will not have aceruloplasminemia or be a carrier pattern has not been see
DIAGNOSIS & TESTING
The diagnosis of aceruloplasminemia is made through a combination of laboratory findings, a brain MRI and an abdominal MRI.
Laboratory findings can include:
- Absence of serum ceruloplasmin (a protein that carries and transports copper)
- Low serum copper concentration
- Low serum iron concentration
- High concentration of serum ferritin (a protein that carries and transports iron)
- Increased iron concentration in the liver
One of the main indications of an aceruloplasminemia diagnosis is evidence of iron accumulation in both the brain and some internal organs. Therefore, in order to correctly diagnose aceruloplasminemia, both brain and abdominal MRIs are necessary. MRI stands for magnetic resonance imaging. An MRI produces a picture of the body that is created using a magnetic field and a computer. The technology used in an MRI is different from that of an x-ray. An MRI is painless and is even considered safe to do during pregnancy. Sometimes an MRI is done of the whole body, but more often, a doctor will order an MRI of particular parts of the body.
Brain and abdominal MRI findings for aceruloplasminemia include:
- Hypointensity (darkness) in the globus pallidus, striatum, thalamus, and dentate nucleus on T2 MRI
- The dark patches indicate iron accumulation
- Iron concentration in the liver is greater than in the brain
Diagnosis of aceruloplasminemia can be confirmed through genetic testing of the CP gene to find two copies of a gene change. Genetic testing is done through sequence analysis, which is able to find the gene change in >92% of cases.
Rarely, an individual with the signs and symptoms of aceruloplasminemia may have only one or no CP gene changes identified. This can happen because the genetic testing is not perfect and has certain limitations. It does not mean the person does not have aceruloplasminemia; it may just mean we do not yet have the technology to find the hidden gene changes. In these cases it becomes very important to have doctors experienced with aceruloplasminemia review the MRI and the person’s symptoms carefully to be as sure as possible of the diagnosis.
MANAGEMENT
 There is no standard treatment for aceruloplasminemia. Patients are managed by a team of medical professionals that recommends treatments based on current symptoms. Chelation therapy should be considered since iron accumulates in both the brain and the body organs.
There is no standard treatment for aceruloplasminemia. Patients are managed by a team of medical professionals that recommends treatments based on current symptoms. Chelation therapy should be considered since iron accumulates in both the brain and the body organs.
After diagnosis, individuals with aceruloplasminemia are recommended to get the following evaluations to determine the extent of their disease:
- Blood work to check for signs of diabetes
- Levels of insulin and HbA1c
The high levels of iron in individuals with aceruloplasminemia can be treated using a variety of therapies and medications including:
- Iron chelating drugs
- Desferrioxamine (given through IV)
- Used in individuals with blood hemoglobin concentration higher than 9 g/dL
- Decreases the concentration of iron in the brain, liver and other visceral organs
- Decreases serum ferritin concentration
- Slows the progression of neurologic symptoms
- Desferrioxamine (given through IV)
- Deferasiox (oral medication)
- Mildly improves cognitive performance, gait and balance
- May be used in individuals who do not respond to desferrioxamine or fresh-frozen plasma therapy (FFP)
- FFP contains ceruloplasmin
- Repeat FFP treatments can improve neurologic symptoms and reduce iron in the liver
- The combination of FFP and desferrioxamine is more effective than FFP alone
- Used along with a chelator or oral administration of zinc
- Prevents tissue damage, particularly to the liver and pancreas
The symptoms of parkinsonism can be treated with the same medications used in Parkinson’s disease. Treatment with dopamine agonist drugs (like levodopa) must be started and monitored carefully. In the beginning, the dose is increased gradually until both the patient and doctor feel symptoms are under control. While taking dopaminergic drugs, individuals must be regularly monitored for adverse neuropsychiatric effects, psychiatric symptoms and worsening of parkinsonism. The benefits of the medication usually only last a few years and are eventually limited by the development of disabling dyskinesias (difficulty performing voluntary movements).
Even after a diagnosis has been made and the appropriate therapies have been decided, it is recommended to continue long-term surveillance to decrease the impact of aceruloplasminemia symptoms and increase quality of life.
Long-term surveillance for aceruloplasminemia can include:
- Regular eye exams to monitor for retinal degeneration
- Annual glucose tolerance test to check for signs of diabetes
- Started at age 15 or as soon as diagnosis is made
- Done early in the course of the disease
- Used to look for signs of cardiac failure from iron accumulation in the heart muscle
PROGRESSION
In most individuals, the three major symptoms (retinal degeneration, diabetes mellitus, and neurologic disease) first appear in adulthood.
The average lifespan varies for individuals with aceruloplasminemia, but due to improvements in medical care, more affected individuals are now living well into late adulthood.
Copyright © 2014 by NBIAcure.org. All rights reserved.